선천 심장혈관 기형(선천 심장 혈관 병/선천성 심장혈관 질환), Congenital cardiovascular diseases
선천(성) 심장혈관 기형의 개요
- 소아청소년들의 심장혈관 질환은
-
- 타고날 때부터 가진 선천(성) 심장혈관 질환과
- 출생 이후 생긴 후천(성) 심장혈관 질환 두 분류로 나눌 수 있다.
- 과거에는 A군 베타 용혈성 연쇄상구균 감염병(A군 연구균)으로 생긴 인두염, 편도염 또는 인두편도염 등을 앓다가 류마티스 열(Rheumatic fever) 및, 또는 류마티스 심장염, 류마티스 관절염 등이 발병했다.
- 그러나 요즘 A군 연구균 감염성 인두염, 편도염, 또는 인두편도염이 발병되면 조기에 적절히 진단 치료하고 잘 예방 해주기 때문에 류마티스 열이나 류마티스 심장병은 드물다.
- 또한 임신, 분만 건강관리를 잘 하고,
- 미숙 신생아들과 만막 신생아들을 건강하게 잘 양육하고,
- 감염병에 걸리지 않게 예방접종을 잘 하고 감염병에 걸리면 신속히 적절히 진단 치료하고,
- 선천성 심장혈관 질환이 있으면 조기에 정확하게 진단 치료를 할 수 있다.
- 분만 전 태아 초음파 검사 등으로 선천 심장혈관 질환을 태어나기 전 진단 치료하기도 하고
- 선천 심장혈관 질환을 가지고 태어나자마자 적절히 치료 할 수 있게됐다.
- 소아청소년의 후천성 심장혈관 질환의 발병률은 점차로 줄어들고 대신 소아청소년 선천 심장혈관 질환이 소아청소년과에서 더 문제시되고 있다.
- 그래서 소아청소년의 후천성 심장혈관 질환의 진단 치료 예방하는 문제보다 선천 심장혈관 질환에 관련된 진단 치료 예방에 관한 문제가 훨씬 더 문제시되고 있다.
- 전보다 대부분의 선천 심장혈관 질환을 심장 수술로 쉽게 완치시킬 수 있게 되었다.
- 통계에 의하여 신생아 1,000명 중 8명이 선천 심장혈관 질환을 갖고 태어난다고 한다.
- 아직도 선천성 심장혈관 질환을 비롯한 신체 다른 계통의 다른 장기에 생긴 선천성 기형은 1세 전 영아들의 사망 원인의 주가 된다. 즉 1세 이전 영아사망의 원인들 중 50%는 선천 심장혈관 질환이다.
- 이런저런 이유로 선천성 심장혈관 질환의 조기진단, 적절한 내외과적 치료, 예방 등에 관해 심장혈관계 질환을 가진 환아들의 부모들은 물론이고 소아 청소년과 전문의,, 소아 심장 내외과 전문의들은 더 많은 관심을 갖게 되었다.
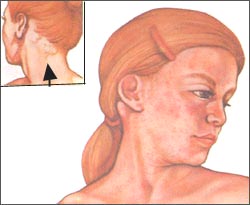
그림 12. 임신 중 풍진바이러스 감염을 비롯한 다른 종류의 바이러스성 감염으로 태아가 감염되어 선천성 심장혈관 질환이 태아에게 생길 수 있다.
Copyright ⓒ 2011 John Sangwon Lee, MD, FAAP

사진 13. 임신부가 타리도마이드제나 다른 어떤 종류의 약물로 치료 받거나 방사능에 노출되면 태아에게 선천 심장혈관 질환이 생길 수 있다.
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
선천 심장혈관 기형의 원인
1. 유전, 염색체 이상, 약물치료, 방사능 노출
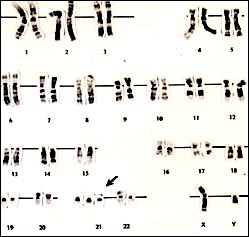
그림 14. Trisomy21(다운 증후군) 염색체
염색체 이상으로 선천성 심장혈관 질환이 생길 수 있다. 다운(Down) 증후군이 있으면 선천성 심장혈관 질환이 생길 수 있는 빈도가 40~50%이다.
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
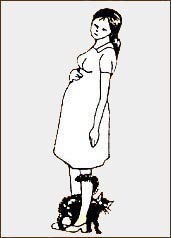
그림 15. 임신 중 태아 톡소플라스마 원충 감염으로 태아에게 선천 심장혈관 질환이 생길 수 있다.
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
- 이상 설명한 바와 같이 임신부가 방사능에 노출되거나,
- 풍진바이러스에 감염되거나
- 그 외 다른 종류의 바이러스에 감염된 태아에게 선천 심장혈관 질환이 생길 수 있다.
- 그렇지만 대부분의 선천 심장혈관 질환의 원인은 확실히 알 수 없다.
- 임신 첫 3개월 기간 중 태아가 풍진바이러스, 콕삭키바이러스, 볼거리바이러스, 사이토메갈로 바이러스 등 바이러스, 또는 톡소플라스마 원충 등 원충에 감염되면 선천 심장혈관 질환이 생길 수 있다.
- 임신 중 임신부의 간질을 치료하기 위해 섭취한 약물이나 다른 종류의 질병을 치료하기위해 쓴 약물로 인해 태아에게 선천 심장혈관 질환이 생길 수 있다. 선천성 심장혈관계 질환 이외 다른 계통의 장기에 선천 질환이 생길 수 있다. [부모도 반의사가 되어야 한다-소아가정간호백과]-제 7권 소아청소년 감염병-풍진, 톡소플라스마증 참조.
- 타리도마이드제 치료를 받았던 임산부들에게 태어난 신생아들에게 여러 종류의 선천성 기형이 생겼다.
- 임신 첫 3 개월 기긴 동안 생긴 임신 우울증을 치료 받았던 임신부들에 태어난 신생아들에게 심실 중격막 결손이 보통 이상으로 많이 발견됐다(Journal watch, BMJ, September 25, 2009).
- 호르몬제 치료를 받았던 임산부들이나 방사능에 노출되었던 임산부에게 태어난 신생아들에게 선천 심장혈관 질환 및, 또는 심장혈관계 이외 다른 계통의 다른 기관에도 선천성 기형이 생길 수 있다.
- 신생아 1천 명 중 8명이 선천 심장혈관 질환을 갖고 태어난다.
- 그러나 친 부모 형제자매들 중 누군가에게 선천 심장혈관 질환을 가진 병력이 있으면 다른 친 형제자매가 선천 심장혈관 질환을 갖고 태어날 가능성이 좀 더 많다.
- 선천 심장혈관 질환을 가진 부모들의 자녀들 1천 명 중 14∼22명이 선천 심장혈관 질환을 갖는다.
- 여러 종류의 선천 심장혈관 질환을 가진 아이들은 심장혈관계 이외 신체의 다른 계통의 장기에도 다른 종류의 선천성 기형을 더 가질 수 있다.
- 때로는 친 형제들이 가진 선천 심장혈관 질환의 종류에 따라 장차 태어날 친동생에게 생길 수 있는 선천 심장혈관 질환의 종류도 미리 추정할 수 있다.
- 요약하면, 대부분 선천 심장혈관 질환의 원인은 확실히 모른다. 그러나 임신 중 임신부에 생긴 감염병, 임신 중 치료에 쓴 약물, 방사능 노출 등으로 태아 선천 심장혈관 질환이 생길 가능성이 있고, 그 외 유전이나, 염색체 이상 등으로 태아 선천 심장혈관 질환이 생길 수 있다. 표 1에 있는 증후군이 있을 때 선천 심장혈관 질환이 생길 수 있다.
선천성 심장혈관 기형 동반 증후군과 질환
표 1. 선천 심장혈관 기형을 동반하는 증후군
| 증후군의 종류 | 선천성 심장기형의 종류 |
| 뇌간신 증후군(Cerebrohepatorenal syndrome, Zellweger syndrome) | 심장 중격결손증을 동반하거나 동반하지 않는 동맥관 개존 |
| 홀트-오람 증후군 (Holt-Oram syndrome) | 심방중격 결손증과 다른 종류의 선천성 심장기형 |
| 후를러 증후군( Hurler’s syndrome) | 심근장애 |
| 프리드라이히 운동실조( Friedreich’s ataxia) | 심근장애 |
| XXXXX 증후군( XXXXX syndrome) | 동맥관 개존 |
| 카펜터 증후군(Carpenter syndrome) | 동맥관 개존증, 심실중격 경손증 등 |
| 코넬리아 다란지 증후군(Cornelia de Lange syndrome) | 선천성 심장 기형이 생기나 일정한 종류의 선천성 기형이 생기지 않는다. |
| 묘성 증후군( Cat cry syndrome/cri-du-chat syndrome) | 선천성 심장 기형이 생기나 일정한 종류의 선천성 기형이 생기지 않는다 |
| 엘리스-반 크레벨트 증후군 (Ellis-van Creveld syndrome) | 중격 결손증 |
| 요골측 무형성증과 혈소판 감소증 (Radial aplasia and thrombocytopenia) | 선천성 심장 기형이 생기나 일정한 종류의 선천성 기형이 생기지 않는다 |
| 클라인펠터 증후군( Klinefelter Syndrome) | 동맥관 개존 |
| 로렌스-문(-바르데)-비들 증후군 (Laurence-Moon(-Bardet)-Biedl syndrome) | 활로사징 |
| 터너 증후군 (Turner syndrome) | 선천성 심장 기형이 생기나 일정한 종류의 선천성 기형이 생기지 않는다 |
출처 및 참조문헌;
-
Nelson text book, 15 edition
- Neonatology Diseases of the fetus and infant, edited by Richard E. Behrman, p.243
- Recognizable patterns of Malformation, Smith Atlas of retardation Symptoms, USA
선천 심장혈관 기형의 종류
1.심장, 혈관 내 비정상 혈류의 유무에 따라 선천성 심장혈관 질환을 분류할 수 있다.
1) 정상 혈액 순환(그림1~6, 10 참조).
- 전신을 순환하던 모든 혈액은 상대정맥과 하대정맥을 통해 우심방 속으로 돌아온다. 그 혈액은 우심방→우심실→폐동맥→폐→폐정맥→좌심방→좌심실→대동맥 속을 거쳐 전신으로 되돌아가는 것이 정상 혈액 순환 과정이다.
- 심방 중격 결손, 심실 중격 결손, 삼천판 폐쇠 등, 심장 내 선천성 심장혈관 질환의 종류에 따라
- 심장에 연결되어 있는 대동맥 협착, 대동맥축착, 폐동맥 협착 등 선천 심장혈관 질환으로 혈액 순환 이상이 생길 수 있다.
- 심방 중격 결손증만 있을 때 우심방 속 혈액이 우심방 속에서 좌심방 속으로, 좌심방 속에서 우심방 속으로 비정상적으로 순환될 수 있다.
- 심실 중격 결손증 있을 때
-
- 심실 중격 결손만 있을 때, 우심실 속에 있는 정맥혈이 폐동맥 속을 거쳐 폐 속으로 흘러 들어간 후 폐정맥→좌심방 속→죄심실 속으로 흘러가기도 하고
- 심실 중격 결손과 폐동맥 협착이 동시 있을 때, 우심실 속에 있는 정맥혈이 우심실 속에서 좌심실 속으로 흘러 들어가 좌심실 내 동맥혈과 섞인 후 대동맥을 거쳐 전신으로 흘러갔다가 전신에서 대정맥을 거쳐 우심방 속으로 되돌아온다. 이 때 전신성 청색증이 생길 수 있다.
- 폐동맥의 일부나 대동맥의 일부가 막혔을 때나, 또는 폐동맥의 일부나 대동맥의 일부가 완전히 막혔을 때 심장 내 피가 정상적으로 순환하지 않고 심장 혈류가 역류되어 비정상 심장내 혈액 순환이 생길 수 있다.
- 대동맥 기시부가 좌심실에서 시작하는 것이 정상인데 대동맥 기시부가 우심실에서 시작하는 선천성 심장 기형도 있다. 이때 전체 심장 혈관 내 혈액 순환에 큰 이상이 생긴다.
한 가지 선천성 심장혈관 기형과 두 가지 선천성 심장혈관 기형
- 좌심실이 없는 선천성 심장 기형도 있다.
- 한 종류의 선천 심장 기형만 있는 경우,
- 여러 종류의 선천 심장 기형 및 질환이 함께 생겨 있는 경우도 있다.
- 여러 번 심장 수술로 완치될 수 없는 선천성 심장혈관 질환도 있고,
- 단 한 번 간단한 심장 수술로 완치될 수 있는 선천 심장혈관 질환도 있다.
- 때로는 심장 내과와 심장 외과의 치료로 완치 할 수 없는 선천 심장혈관 질환도 있다.
선천성 심장혈관 기형이 있는 심장 혈관 위치와 선천성 심장혈관 기형의 수에 따라 선천성 심장혈관 기형을 분류할 수 있다.
- 심장의 어느 부분에 선천성 심장혈관 기형이 생겨 있느냐,
- 선천성 심장혈관 기형이 좌심실에서 시작하는 대동맥에 생겼는냐, 그렇다면 대동맥 어느 부분에 생겼느냐
- 우심실에서 시작되는 폐동맥의 어느 부분에 기형이 생겨 있는지,
- 선천성 심장혈관 기형의 크기는 어느 정도인지,
- 얼마나 심한 선천성 심장혈관 기형인지,
- 한 종류의 선천성 심장혈관 기형만 생겨 있는지,
- 두 종류의 선천성 심장혈관 기형이 생겨 있는지,
- 2개 이상 여러 종류의 심장혈관 기형이 동시 생겨 있는지
등에 따라 선천성 심장혈관 기형을 분류할 수 있다.
비청색증 형 선천성 심장혈관 기형과 청색증 형 선천성 심장혈관 기형으로 분류할 수 있다.
- 전신성 청색증이 선천성 심장혈관 기형으로 생기는지, 전신성 청색증이 생기지 않는지에 따라 선천성 심장혈관 기형을 청색(증) 형 선천성 심장혈관 기형과 비청색증 형 선천성 심장혈관 기형으로 분류하기도 한다.
- 좌심실 내 동맥혈이 대동맥을 통해 전신으로 흘러가는 것이 정상 혈액 순환이다.
- 전신성 청색증 형 선천성 심장혈관 기형이 있을 때는 심장의 좌심실 속에서 순 정맥혈, 또는 정맥혈과 동맥혈이 섞인 혼합 정맥 동맥혈이 전신으로 흘러갈 수 있다.
- 이 경우, 전신에 청색증이 생길 수 있고 그로 인해 입술, 혀, 손톱 밑, 그 외 신체 다른 각 부위에도 청색증이 생길 수 있다. 이와 같이 전신성 청색증을 동반 할 수 있는 선천성 심장혈관 기형을 전신성 청색증 형 선천성 심장혈관 기형이라고 한다.
- 우심방 속에 있는 정맥혈이 삼천판을 통과해서 우심실 속을 거쳐 폐동맥을 통과한 후 폐 속으로 흘러가는 것이 정상 혈액순환이다.
- 그러나 우심방 속에 있는 정맥혈이 우심실 속을 거쳐→ 폐동맥을 거쳐 폐 속으로 흘러가지 않고 심방 중격 결손 등을 거쳐 좌심방 속으로 흘러들어간 다음 전신으로 순환되는 선천성 심장혈관 기형이 있을 때는 중추성 청색증(Central cynosis)이 생길 수 있다.
- 중추성 청색증이 생기지 않는 선천성 심장혈관 기형을 비청색증 형 선천성 심장혈관 기형이라고 한다.
- 다시 설명하면, 심장이 동맥혈을 전신에 보낼 수 있고 피부나 점막에 중추성 청색증이 생기지 않는 선천성 심장혈관 기형을 비청색증 형 선천성 심장혈관 기형이라고 한다.
선천성 심장혈관 기형의 증상 징후
- 선천성 심장혈관 기형의 정도, 종류, 선천성 심장혈관 기형으로 인한 합병증의 유무, 나이 등에 따라 증상 징후가 다르다.
- 요즘 대부분의 신생아들이 병원 분만실에서 태어난 후 신생아실 양호를 받고 집으로 퇴원하기 전에 적어도 한두 번 정도 정밀 신생아 건강검진을 적어도 1~3회, 소아청소년과 전문의로부터 받기 때문에 대부분의 선천성 심장혈관 기형은 신생아실 신생아 건강검진을 받을 때 진단받아 적절한 치료를 바로 받는 것이 보통이다.
- 비록 신생아실에서 신생아 건강검진을 받을 때 선천성 심장혈관 기형이 있는 것을 진단받지 못했어도 신생아실에서 집으로 퇴원한 후 3~14일 첫 정기 건강검진을 소아청소년과에서 검진 받을 때나 태어나서부터 사춘기가 될 때까지 소아청소년들(0~18 세)이 건강검진을 정기적으로 받는 거시 보통이다. 태어날 때부터 가지고 있던 신생아들이나 영아들의 선천성 심장 기형 등을 조기에 진단받을 수 있고 조기에 적절히 치료받을 수 있는 것이 보통이다.
- 어떤 종류의 선천성 심장혈관 기형은 타고날 때도 있었지만 아무 증상 징후가 나타나지 않을 수 있다.
- 부모가 자녀에게 어떤 선천성 심장혈관 기형이 있는지 모르고 있다가 다른 어떤 종류의 병으로 소아청소년과에서 건강 검진을 받는 동안 또는 학교 정기 건강검진을 받는 중 비정상 심 잡음을 처음 듣고서 선천성 심장혈관 질환이 있다는 사실을 처음 진단받는 경우도 있다.
- 심한 선천성 심장혈관 기형의 대부분은 출생 후 그 선천성 심장혈관 기형으로부터 생긴 증상 징후가 곧 나타나는 것이 보통이다.
- 그 때문에 출생 후 선천성 심장혈관 기형이 있다는 것을 조기에 진단받는 것이 보통이다.
- 때로는 신생아기에 선천성 심장혈관 기형이 있다는 것을 진단받지 못 할 수 있다. 그러나 심한 선천성 심장혈관 기형이 있을 때 대부분의 경우 여러 가지의 증상 징후가 신생아기 때부터 나타나기 때문에 적어도 생후 1~2개월 이전에 심한 선천성 심장혈관 기형이 있다고 처음 진단받는 것이 보통이다.
- 심한 선천성 심장혈관 기형이 있으면 신생아들이나 영유아들의 맥박이 빠르고 숨을 자주 쉬고 얼굴이 창백한 증상 징후가 나타난다.
- 젖을 빨아먹는 데나 인공영양을 빨아먹는 데도 힘들여 빨아 먹고 오래 걸려 먹는다.
- 체중이 잘 늘지 않고 성장 발육지연이 될 수 있고 생기가 없어 보일 수 있다.
선천성 심장혈관 기형의 진단
- 병력, 증상 징후, 진찰소견 등을 종합해 선천성 심장혈관 질환이 있다고 의심되면 가슴 X-선 사진, 심전도, 심장혈관 초음파 검사, 심장 핵의학 검사, 심장 혈관 MRI, 심장 카테터 검사, 그 외 다른 여러 종류의 검사로 진단할 수 있다.
- 선천성 심장혈관 기형의 종류, 정도, 합병증의 유무, 나이 등에 따라 진단 방법이 다르다.
- 경미한 선천성 심장혈관 기형을 가진 아이들의 일부는 선천성 심장혈관 기형이 있는 줄도 모르고 일생동안 건강하게 살 수 있다.
- 심한 선천성 심장혈관 기형을 가진 아이들 중 어떤 아이는 선천성 심장혈관 기형으로 인해 평소에 보통 일상생활을 제대로 하지 못하고 선천성 심장혈관 질환으로 생긴 합병증 때문에 많이 고생한다.
- 갓 태어난 신생아의 심한 선천성 심장혈관 기형을 신생아실에서 응급 진단 치료를 받고 종합 병원 신생아 집중치료실에서 추적 응급 수술 치료를 받고 살아나는 경우도 있다.
- 선천성 심장혈관 기형이 있다고 의심되면 가슴 X-선 사진검사, 심전도 검사, 심장 심초음파(에코카디오그램)검사, 심장 도자법(심장 카세테리제이션), 심음도(포노카디오그램)검사 및, 또는 그 외 다른 여러 가지 검사로 확진할 수 있다.
- 이런 검사로 진단하기 전에 시진, 촉진, 타진, 청진 등으로 심장을 진찰하는 것이 기본이다.
- 요즘 선천성 심장혈관 질환을 진단하는 의술이 눈부시게 발달되어 심한 선천성 심장 기형을 태어난 바로 그날 금방 쉽게 진단하는 것이 보통이다.
- 심장에 붙어있는 대동맥이나 폐동맥 등에도 선천성 혈관 기형이 생길 수 있다.
- 대동맥이나 폐동맥의 기시부가 붙어있는 심장 부분 판막 등에 어떤 기형이 생겨 있는지 대동맥이나 폐동맥의 어느 부분에 기형이 생겼는지 있다면 그 크기는 어느 정도인지, 그 기형의 해부학 구조는 어떤지, 대동맥이나 폐동맥과 심장의 기능이 정상적인지 등을 정확히 진단할 수 있고
- 그 상세한 진단 결과에 따라 선천성 심장혈관 기형이나 대동맥이나 폐동맥 기형을 효과적으로 치료할 수 있다.
- 대부분의 선천성 심장혈관 기형을 비교적 안전하고 쉽게 수술로 완치시킬 수 있다.
- 그러나 일부의 선천성 심장혈관 기형은 완치되지 않는다.
- 완치시키기가 불가능한 선천성 심장혈관 기형은 심장 혈관의 기능이 정상을 할 수 있게 고식적 심장 수술 치료(Palliative surgery treatment)를 한다. 선천성 심장혈관 기형은 조기에 확진해서 조기에 적절히 치료해야 한다.
- 맥박 산소측정으로 신생아 무증상 심한 선천성 심장 혈관 기형을 진단할 수 있다고 한다(Pulse oximetry detects heart defects in newborns . 소스 : :Contemporary Pediatrics eConsult, May 17, 2012.
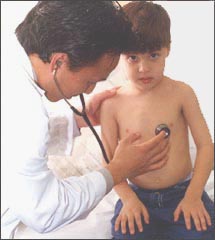
사진 16. 병력, 증상 징후, 진찰 등으로 선천성 심장 기형을 진단할 수 있다
Copyright ⓒ 2011 John Sangwon Lee, MD, FAAP
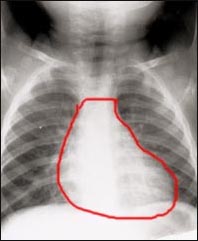
사진 17. 가슴 X-선 사진은 선천성 심장 기형을 진단하는데 많이 도움 된다. 붉은 원내 하얀 부위가 심장이다
Copyright ⓒ 2011 John Sangwon Lee, MD, FAAP
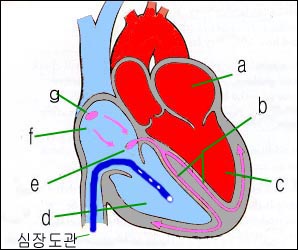
그림 20. 하 대정맥을 통한 심도자법 (심장도자법, 심장 카세테리제이션)
Copyright ⓒ 2011 John Sangwon Lee, MD, FAAP
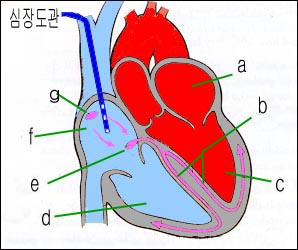
그림 21. 상 대정맥을 통한 심도자법 (심장도자법, 심장 카세테리제이션)
a-좌심방, b-히스 속, c-좌심실, d-우심실, e-3천판, f-우심방, g-동방결절
Copyright ⓒ 2011 John Sangwon Lee, MD, FAAP
선천성 심장혈관 기형의 치료
- 선천성 심장 기형의 크기, 증상 징후, 종류, 합병증, 환아의 나이 등에 따라 다르게 치료한다.
- 아주 작은 심실 중격 결손, 아주 작은 미숙아에게 생긴 동맥관 개존, 그 외 어떤 종류의 선천성 심장 혈관 기형은 심장 수술 치료를 받지 않아도 자연히 나을 수 있다.
- 때로는 아무 증상 징후도 없이 별다른 치료를 받을 필요 없이 그 선천성 심장혈관 기형을 일생동안 가지고 정상적으로 살 수 있다.
- 소아청소년과에서 어떤 종류든 선천성 심장혈관 기형이 있다는 진단을 받으면 곧 소아 심장내과 전문의로부터 더 확실한 진단 치료를 곧 받아야 한다.
- 선천성 심장혈관 기형이 있거나, 좌심실 대동맥 기시부분 또는 우심실 폐동맥 기시부분 등에 선천성 기형이 있을 수 있다. 이때 그 기형이 심장 기시부분 중 어떤 부분에 생겨 있는지 더 확실히 자세히 진단받아야 한다.
- 그 선천성 심장혈관 기형을 심장 수술로 치료받아야 하는지,
- 심장 수술 치료를 받을 필요가 없는지,
- 심장 수술 치료로 완치될 수 있는지,
- 1차 심장 수술 치료를 받아 완치 시킬 수 있는지, 2차적 심장 수술 치료를 받아야 완치 할 수 있는지, 심장 수술 치료를 받아도 완치될 가능성이 없는지 등등 선천성 심장 혈관 기형 수술 치료에 관한 정보를 속히 자세히 알아야 한다.
- 심장 수술 치료를 받아야 할 때는 언제, 어디서, 어떤 소아 심장외과 전문의로부터 수술치료를 받을 것인지,
- 수술 치료를 받기 전에 어떤 약물로 예방적 치료를 받아야 할 것인지,
- 심장 수술 치료의 성공률은 얼마인지,
- 심장 수술 치료에 소요되는 진료비용은 얼마인지,
- 수술을 받은 후의 예후는,
- 천성 심장혈관 기형을 가진 환아와 부모가 평소에 주의 할 사항 등에 관해 가능한 한 속히 알아야 한다.
- 국가 사회 복지 보험에서 진료비 혜택을 받을 수 있는지
- 부모는 적어도 소아 선천성 심장혈관 기형에 관해 반의사가 되어야할 지식이상 더 많은 의학지식을 가져야 한다.
- 선천성 심장혈관 기형을 수술로 치료받을 때는 소아 심장내과 전문의, 소아 심장외과 전문의, 소아청소년과 전문의와 그 밖에 다른 여러 전문의, 소아 심장혈관 기형 전문 간호사, 임상병리요원 등이 선천성 심장혈관 기형 치료 팀 멤버가 되어 성공적으로 수술을 마치는데 동참하는 것이 보통이다.
- 이런 이유로 선천성 심장혈관 기형 수술 치료는 아무 병원에서 할 수 없고 전국 몇몇 종합 병원에서만 하는 것이 보통이다.
- 선천성 심장혈관 질환에 관해서 더 자세한 정보는 다음 각 항에서 참조한다.
- 성인의 심장 기능 상실(Heart failure) 치료에 쓰는 ivabradine(Corlanor)으로 소아 심장 기능 상실을 치료 하기도 한다. 소스: AAP News 6/2019
출처 및 참조문헌
-
심실 중격 결손(Ventricular septal defect)
- 심방 중격 결손(Atrial septal defect)
- 동맥관 개존(Patent ductus arteriosus)
- 대동맥 축착(Coarctation of aorta)
- 대동맥 협착(Aortic stenosis)
- 폐동맥 협착(Pulmonary stenosis)
- 활로 4징(Tetralogy of Fallot)
- 삼첨판 폐쇄(Tricuspid atresia)
- 대혈관 전위(폐동맥과 대동맥의 전위 (Transposition of the great arteries)
|
다음은 “심방중격 결손증, 심실심방 중격 결손증, 선천성 심장 기형, 좌 수신증”에 관한 인터넷 소아청소년 건강상담 질의응답의 예 입니다. |
Q&A.심방중격 결손증, 심실심방 중격 결손증, 선천성 심장 기형, 좌 수신증
Q.
안녕하십니까? 저는 29세의 남성으로서 일본에 거주하고 있습니다. 다름이 아니오라 아내(일본인)8월 12일 남자아기를 출산하였는데 병원에서 심실/심방 중격 결손증과 수신증 진단을 내렸습니다. 심실 중격 결손증의 위치는 폐동맥 바로 아래이고 심방 중격 결손증의 위치는 대동맥에서 좀 떨어진 곳이라고 합니다. 심방 중격 결손증의 천공크기는 아직 명확히 진단을 못 내렸으나 심실 중격 결손은 가로 6미리 세로 3미리로 측정을 하였습니다. 수신증은 좌측 신우 한쪽이 비정상적인 크기라고 진단했으며 우측의 정상신우의 1.5~1.8배라고 합니다.
출산 전 초음파로 수신증은 체킹이 되어서 경과를 지켜보면서 치료계획을 세우기로 하였으나
심장 기형은 출산 후 신장검사를 위한 정밀검사 도중 체킹된 것입니다
기타사항
– 임신 5개월 차에 임신사실을 알고 병원에 갔습니다(입덧이 전혀 없었음).
– 산모가 무월경현상을 임신이라고 생각지 않고 병원에 진료를 받으러 가지 않았습니다.
– 임신 1~-2개월 차의 기초 태아검사는 받지 않았습니다(각종 기형 체크 등).
– 24주차, 30주차에 걸쳐 2차례의 역아현상이 있었습니다.
– 출산예정일 3주일 전에 입원을 하여 태아의 심박체크를 하면서 제왕절개 준비를 하다가
3회 때의 심박급상승 후 의사의 진단 하에 제왕절개를 시행하였습니다.
아기의 현재상태(8일차)
– 배뇨 이상없음
– 혈압, 심박등 바이탈 사인 이상없음(병원으로부터 진단)
– 하루에 1회 1분-2분정도 심박 100이하로 떨어지는 현상 있음
– 모유를 제 힘으로 잘 먹지 못함. 모유는 1회 5cc 이하 밖에 빨지 못함
– 인공유는 1회 40-50cc 1일 4~5회에 걸쳐서 먹임
– 수유시간에도 먹지 않고 잠만 자는 경우가 있었음(간호사가 아무리 깨워도 안 일어납니다)
좀 길어지긴 했지만 신장뿐만이 아니라 심장 쪽의 이상도 발견되게 되어 참으로 걱정이 많습니다. 조기에 발견된 데 대해서는 다행으로 생각하지만 신생아에게 고통스러운 일이 아닌지 참으로 가슴이 아픕니다. 이쪽 의료진에서는 수술을 최악의 경우로 잡고 앞으로 2~3주 후 경과를 더 지켜보면서 정밀검사를 행하겠다는 치료계획을 통보해 주었습니다. 여러 가지 말을 많이 들으면서 안심하라는 말을 듣고 또 개인적으로 홈페이지를 찾아보면서 어중이 떠중이 식으로 알아는 보았지만 역시 중격 결손이 심실심방 두 군데나 있는 것으로 미루어 보아 수술의 가능성이 높아지고 있습니다. 막 태어난 아기에게 수술을 시킨다는 것이 결과적으로는 좋을지 몰라도 초보아빠엄마의 입장에서는 너무나도 불안하고 아기가 안쓰럽습니다.
괜찮을까요? 저는 앞으로 어떤 준비를 해야 할까요?
A.
대디님께
안녕하세요.
좋은 질문과 상세한 병력을 주셔서 대단히 감사합니다. 선생님께서 주신 가족병력, 과거병력, 임신병력, 출산과정, 진단 등을 주셔서 또 한번 감사를 드립니다.
아기자녀의 탄생을 축하드립니다.
이렇게 훌륭하신 부모님을 가진 아기는 곧 하나님의 영광과 축복을 받고 곧 회복될 것입니다.
너무도 심한 선천성 심장혈관 기형을 가지고 있던 환아들이 심장혈관 기형 치료 수술을 받은 후 건강하게 정상적으로 성장하는 것을 보면 얼마나 마음이 흐뭇하고 기뻤는지 모릅니다.
제가 미국 예일대학 의과 대학 소아과 병원과 Uconn 의과대학 소아과와 하트포드 병원에서 경험했던 일들입니다.
요즘 대부분의 선천성 심장혈관 기형을 조기에 정확하게 진단할 수 있고 선천성 심장혈관 기형 치료 수술 및 내과적 치료로 비교적 쉽게 완치 할 수 있고 또 수술은 받은 후 추적치료도 잘할 수 있습니다.
위중한 병을 앓는 자녀나 부모 본인에게 FAGS 증후군이 생길 수 있지만 너무 걱정을 하시지 마시고 의사 선생님의 지시에 따라 계속 보살피고 치료해 주시면서 기도 하십시오
저는 대디 선생님은 비 의료인인 부모이시든지 의사이시든지 의학에 관해, 특히 소아과학에 조예가 깊으신 분이라고 생각합니다.
제가 몇 말씀을 드리고자 합니다.
저도 질문을 받고 더 공부를 하고 정리 해 보겠습니다.
심방중격 결손증을 크게
난원공 개존,
이차공 결손,
심내막 융기 결손 등으로 분류합니다. (심방 중격 결손증 참조)
난원공 개존은 선천성 심장 기형이 아닙니다.
난원공 개존은 폐동맥 폐쇄나 삼천판 폐쇄가 없고 또 어떤 선천성 심장 혈관 기형이 우심실에 있지 않는 한 자연적으로 막히는 것이 정상입니다.
때로는 난원공 개존 현상이 일생동안 그대로 있을 수 있고 건강에 문제가 되지 않습니다.
이차공 결손이나 심내막상 결손의 크기와 증상 징후에 따라 소아청소년과 전문의, 소아 심장내과 전문의, 소아 심장외과 전문의와 그 외 다른 전문의의 치료를 바로 받아야 합니다.
좌 수신증의 원인이 무엇인지 알아야 하겠습니다.
신체의 한 계통에 선천성 기형이 있으면 신체의 다른 계통에 다른 종류의 선천성 기형이 잇을 가능성이 있습니다.
예를 들면 다운 증후군이 있는 환아에게 선천성 심장혈관 기형이 있을 수 있고, 방광 요로역류가 있을 수 있고 그로 인해 수신증이 생길 수 있습니다. 그에 대한 적절한 진단치료를 받으시기 바랍니다.
이렇게 치료를 해보시는 것이 어떨지요.
영양분과 수분, 전해질 등에 어떤 이상이 생기지 않게 영양분 섭취를 잘 해야 합니다.
소아 간호사와 영양사의 도움을 받으면 좋을 것입니다.
빈혈이 있는지 알아보시기 바랍니다.
아시겠지만 선천성 심장혈관 기형 특히 전신성 청색증이 있는 경우, 헤모글로빈 농도가 심장혈관 기형이 없는 갓 태어난 신생아들이나 영유아들의 헤모글로빈 농도에 비해 더 높은 것이 정상입니다. 그런 이유로 헤모글로빈 농도가 정상치 일지라도 빈혈에 걸려 있을 수 있습니다.
선천성 심장혈관 기형으로 전신성 청색증이 생길 수 있습니다.
전신성 청색증이 있으면 산소호흡 치료를 받아야 할 때도 있습니다.
전신성 청색증이 있으면 적혈구 수치가 정상 보다 더 높을 수 있습니다.
심장 울혈증이 생길 수 있고 폐렴 등 감염병에 더 잘 걸릴 수 있습니다.
구강 등 소화기계통이나 다른 계통에 있는 신체 부위를 수술 받을 때 심내막염에 더 쉽게 걸릴 수 있습니다. 그래서 항생제 예방적 치료를 받아 해야 합니다.
선천성 심장혈관 기형과 수신증이 왜 생겼는지 원인을 알기 위해 유전학 전문의와 상담하시고 염색체 검사를 하는 것도 고려해야합니다.
소아청소년과 전문의, 소아 신장내과 전문의, 소아 신장외과 전문의의 도움을 받아 수신증의 원인을 알아보고 여러 가지 비뇨기계 질환을 진단하는데 필요한 검사를 하고 그에 따라 적절한 치료를 받아야 합니다.
요로 감염에 걸리지 않게 예방적 치료를 해야 합니다.
각종 기본 예방접종을 나이와 시기에 맞춰 접종 받아야 합니다.
가능하면 각종 건강보험을 들어놓으시기 바랍니다.
아기의 모든 건강 문제는 담당 소아청소년 전문의와 상의해서 결정하시는 것이 좋습니다.
이상 설명한 것 외에 아기자녀를 위해서 특별히 해야 할 일이 더 많이 있습니다.
더 필요하면 단골 소아청소년과 의사와 상담하시기 바랍니다.
아시겠지만 저는 일반 소아과 전문의입니다.
소아청소년과는 일반 소아청소년과가 있고 소아청소년과 전문의는 신체의 각 계통에 따라 그 계통 소아과학을 더 특별히 전문으로 공부하고 연구한 각 계통 소아청소년과 전문의로 나누어집니다.
일반 소아청소년과 전문의는 소아과학에 관한 전반적 소아과학을 전문합니다.
일반적인 소아과학을 전문하고 소아 심장에 관한 소아과학을 전문한 소아청소년과 전문의를 소아 심장내과 전문의라고 합니다.
일반적으로 소아청소년과 전문의가 소아 심장혈관 질환에 관해 어떤 의문이 더 있으면 소아 심장을 특별히 전문으로 하는 소아 심장 내과전문의에게 자문해서 그 환아를 보게 할 수 있습니다.
외과도 역시 소아 심장 외과에 관해 특별히 전문한 소아 심장 외과전문의에게 의뢰해서 소아 심장 혈관 질환 수술 등에 관해 상담 치료받게 하는 것이 요즘 진료 의술입니다.
이상 설명한 것 외에 아기자녀를 위해서 특별히 더 해야 할 일이 더 많이 있으니 소아청소년과 의사와 상담하시기 바랍니다.
또 소아들이 수술을 받을 때 소아 마취를 주로 전문하는 소아 마취 전문의가 있고 소아들의 질병을 전문으로 간호해 주는 소아청소년과 전문 간호사도 있습니다.
그뿐만 아니라 소아청소년들만 특별히 입원해 치료 받는 소아청소년 병원도 있고 소아청소년들의 안녕에 관한 제반문제를 보다 효과적으로 다룰 수 있는 소아청소년 병원과 스태프가 있는 소아청소년 병원들이 여기저기에 설립되어 있습니다.
제가 이 말씀을 드리는 이유는 적절한 의료진과 병원을 선정하시는데 도움 되시기를 바라서입니다.
제가 배우는데 도움 되게 치료 결과를 알려주시면 감사하겠습니다. 질문이 더 있으시면 다시 연락 주시기 바랍니다. 감사합니다. 이상원
Congenital cardiovascular diseases
Overview of Congenital (Gender) Cardiovascular Anomalies
Cardiovascular disease in children and adolescents
o Congenital (sexual) cardiovascular disease and
o Acquired (gender) cardiovascular disease occurring after birth can be divided into two categories.
• In the past, patients with pharyngitis, tonsillitis, or pharyngotonsillitis caused by group A beta-hemolytic streptococcal infectious disease (group A research bacteria) developed rheumatic fever, or rheumatoid carditis and rheumatoid arthritis.
• However, these days, rheumatic fever or rheumatic heart disease is rare because group A research bacteria infectious pharyngitis, tonsillitis, or pharyngotonsillitis is diagnosed and treated at an early stage and well prevented.
• Also, take good care of your pregnancy and childbirth health,
• Nurturing premature and full-term newborns in a healthy way,
• Vaccinate well so that you do not get an infectious disease, and if you do get an infectious disease, promptly and appropriately diagnose and treat it;
• If you have congenital cardiovascular disease, you can accurately diagnose and treat it at an early stage.
• Diagnosis and treatment of congenital cardiovascular disease before birth through prenatal ultrasonography, etc.
• Congenital cardiovascular disease can be treated appropriately as soon as it is born.
• The incidence of acquired cardiovascular disease in children and adolescents is gradually decreasing, but congenital cardiovascular disease in children and adolescents is becoming a more problematic issue in the Department of Pediatrics.
• Therefore, the problem of diagnosis and treatment prevention related to congenital cardiovascular disease is much more problematic than the problem of diagnosis and treatment prevention of acquired cardiovascular disease in children and adolescents. • It is now easier to cure most congenital cardiovascular diseases with heart surgery than before. • Statistics show that 8 out of 1,000 newborns are born with congenital cardiovascular disease.
• Congenital anomalies in other organs of the body, including congenital cardiovascular disease, are still the leading cause of death in infants before the age of 1 year. In other words, 50% of the causes of infant mortality before the age of 1 year are congenital cardiovascular disease.
• For various reasons, early diagnosis of congenital cardiovascular disease, appropriate internal and external treatment, and prevention, as well as parents of children with cardiovascular disease, pediatricians, and pediatric cardiologists have become more interested.
Figure 12. Other types of viral infection, including rubella virus infection, during pregnancy, can infect the fetus and cause congenital cardiovascular disease in the fetus. Copyright ⓒ 2011 John Sangwon Lee, MD, FAAP
Photo 13. If a pregnant woman is treated with thalidomide or any other drug or is exposed to radiation, her fetus can develop congenital cardiovascular disease. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
Causes of congenital cardiovascular malformations
1. Genetics, chromosomal abnormalities, drug treatment, radiation exposure
Figure 14. Trisomy21 (Down syndrome) chromosome Chromosomal abnormalities can lead to congenital cardiovascular disease. With Down syndrome, the incidence of congenital cardiovascular disease is 40-50%. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
Figure 15. Fetal Toxoplasma protozoa infection during pregnancy can lead to congenital cardiovascular disease in the fetus. Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
• As described above, if a pregnant woman is exposed to radiation,
• Infected with rubella virus or
• Fetuses infected with other types of viruses may develop congenital cardiovascular disease.
• However, the cause of most congenital cardiovascular diseases is unknown.
• Congenital cardiovascular disease can occur if the fetus is infected with viruses such as rubella virus, coxsackievirus, mumps virus, cytomegalovirus, or protozoa such as toxoplasma during the first trimester of pregnancy.
• During pregnancy, medications taken to treat a pregnant woman’s epilepsy or medications used to treat other types of disease can cause the fetus to develop congenital cardiovascular disease. Congenital diseases can occur in organs other than congenital cardiovascular disease. www.drleepediatrics.com- Volume 7 Infectious diseases in children and adolescents – Rubella, toxoplasmosis.
• Several types of congenital anomalies have occurred in newborns born to pregnant women who have been treated with thalidomide.
• Ventricular septal defects were found to be unusually high in newborns born to pregnant women treated for gestational depression during the first trimester of pregnancy (Journal watch, BMJ, September 25, 2009).
• Pregnant women who have received hormone therapy or newborns born to pregnant women exposed to radiation may develop congenital cardiovascular disease or other congenital malformations in organs other than the cardiovascular system.
• Eight out of every 1,000 newborns are born with congenital cardiovascular disease.
• However, if one of your biological parents or siblings has a history of congenital cardiovascular disease, the other biological sibling is more likely to be born with congenital cardiovascular disease.
• Between 14 and 22 children out of 1,000 children of parents with congenital cardiovascular disease have congenital cardiovascular disease.
• Children with several types of congenital cardiovascular disease may also have other types of congenital anomalies in organs other than the cardiovascular system.
• Sometimes, depending on the type of congenital cardiovascular disease that the siblings have, the type of congenital cardiovascular disease that a future sibling may have can be estimated in advance.
• In summary, the cause of the most congenital cardiovascular diseases is unknown. However, there is a possibility that fetal congenital cardiovascular disease may occur due to infectious diseases that occurred during pregnancy, drugs used for treatment during pregnancy, radiation exposure, etc. Congenital cardiovascular disease may occur when the syndromes listed in Table 1 are present.
Syndromes and diseases with congenital cardiovascular malformations
Table 1. Syndromes with congenital cardiovascular malformations
표 1. 선천 심장혈관 기형을 동반하는 증후군
| type of syndrome | Types of congenital heart anomalies |
| 뇌간신 증후군(Cerebrohepatorenal syndrome, Zellweger syndrome) | 심장 중격결손증을 동반하거나 동반하지 않는 동맥관 개존 patency of the ductus arteriosus with or without cardiac septal defect |
| 홀트-오람 증후군 (Holt-Oram syndrome) | 심방중격 결손증과 다른 종류의 선천성 심장기형 Atrial septal defect and other congenital heart malformations |
| 후를러 증후군( Hurler’s syndrome) | 심근장애 myocardial disorder |
| 프리드라이히 운동실조( Friedreich’s ataxia) | 심근장애 myocardial disorder |
| XXXXX 증후군( XXXXX syndrome) | 동맥관 개존 patency of the ductus arteriosus |
| 카펜터 증후군(Carpenter syndrome) | 동맥관 개존증, 심실중격 경손증 등 Patient ductus arteriosus, ventricular septal insufficiency, etc. |
| 코넬리아 다란지 증후군(Cornelia de Lange syndrome) | 선천성 심장 기형이 생기나 일정한 종류의 선천성 기형이 생기지 않는다. Congenital heart anomalies occur, but certain types of congenital anomalies do not occur. |
| 묘성 증후군( Cat cry syndrome/cri-du-chat syndrome) | 선천성 심장 기형이 생기나 일정한 종류의 선천성 기형이 생기지 않는다 Congenital heart anomalies occur, but certain types of congenital anomalies do not occur |
| 엘리스-반 크레벨트 증후군 (Ellis-van Creveld syndrome) | 중격 결손증 septal defect |
| 요골측 무형성증과 혈소판 감소증 (Radial aplasia and thrombocytopenia) | Congenital heart anomalies occur, but certain types of congenital anomalies do not occur |
| 클라인펠터 증후군( Klinefelter Syndrome) | 동맥관 개존 patency of the ductus arteriosus |
| 로렌스-문(-바르데)-비들 증후군 (Laurence-Moon(-Bardet)-Biedl syndrome) | 활로사징 Fallot 4 signs |
| 터너 증후군 (Turner syndrome) | 선천성 심장 기형이 생기나 일정한 종류의 선천성 기형이 생기지 않는다 Congenital heart anomalies occur, but certain types of congenital anomalies do not occur |
Sources and references;
• Nelson textbook, 15 edition • Neonatology Diseases of the fetus and infant, edited by Richard E. Behrman, p.243
• Recognizable patterns of Malformation, Smith Atlas of retardation Symptoms, USA
Types of congenital cardiovascular malformations
1. Congenital cardiovascular disease can be classified according to the presence or absence of abnormal blood flow in the heart and blood vessels.
1) Normal blood circulation (see Figures 1-6, 10).
• All blood circulating throughout the body returns to the right atrium through the superior vena cava and inferior vena cava. The normal blood circulation process is that the blood returns to the body through the right atrium → right ventricle → pulmonary artery → lung → pulmonary vein → left atrium → left ventricle → inside the aorta.
• Depending on the type of congenital cardiovascular disease in the heart, such as atrial septal defect, ventricular septal defect, or three-thousand plate occlusion
• Congenital cardiovascular diseases such as aortic stenosis, aortic stenosis, and pulmonary artery stenosis, which are connected to the heart, can cause blood circulation abnormalities.
• When there is only atrial septal defect, blood in the right atrium may circulate abnormally from the right atrium to the left atrium and from the left atrium into the right atrium.
• In case of the ventricular septal defect
• o When there is only a ventricular septal defect, the venous blood in the right ventricle flows into the lungs through the pulmonary artery, and then flows into the pulmonary vein → into the left atrium → into the sin ventricle.
o When ventricular septal defect and pulmonary artery stenosis occur at the same time, venous blood in the right ventricle flows from the right ventricle into the left ventricle, mixes with the arterial blood in the left ventricle flows through the aorta, and returns to the right atrium through the vena cava. In this case, systemic cyanosis may develop.
• When a part of the pulmonary artery or part of the aorta is blocked, or when part of the pulmonary artery or part of the aorta is completely blocked, the blood in the heart does not circulate normally and the heart blood flow backs up, resulting in abnormal intracardiac blood circulation.
• It is normal for the aortic origin to originate in the left ventricle, but there are also congenital heart anomalies in which the aortic origin originates in the right ventricle. At this time, a major abnormality occurs in the blood circulation in the entire cardiovascular system.
One congenital cardiovascular malformation and two congenital cardiovascular malformations
• There are also congenital heart anomalies without a left ventricle.
• If you have only one type of congenital heart anomaly,
• Several types of congenital heart anomalies and diseases may coexist.
• There are congenital cardiovascular diseases that cannot be cured with multiple heart surgeries;
• Some congenital cardiovascular diseases can be cured with just one simple heart surgery.
• Sometimes there are congenital cardiovascular diseases that cannot be cured by cardiology and cardiac surgery.
Congenital cardiovascular anomalies can be classified according to the location of the cardiovascular vessels with congenital cardiovascular anomalies and the number of congenital cardiovascular anomalies.
• Which part of the heart has congenital cardiovascular malformations;
• Does the congenital cardiovascular anomaly originate in the aorta originating from the left ventricle and, if so, in which part of the aorta?
• what part of the pulmonary artery that starts from the right ventricle is malformed;
• what is the size of the congenital cardiovascular anomaly;
• how severe the congenital cardiovascular anomaly;
• There is only one type of congenital cardiovascular malformation;
• two types of congenital cardiovascular malformations;
• Whether two or more types of cardiovascular malformations occur simultaneously. Congenital cardiovascular anomalies can be classified according to
It can be classified into a cyanotic type congenital cardiovascular anomaly and a cyanotic type congenital cardiovascular anomaly.
• Depending on whether systemic cyanosis is caused by a congenital cardiovascular malformation or systemic cyanosis does not occur, congenital cardiovascular malformations are sometimes classified into cyanotic congenital cardiovascular malformations and non-cyanotic congenital cardiovascular malformations.
• Normal blood circulation is the flow of arterial blood from the left ventricle to the body through the aorta.
• When there is a systemic cyanotic congenital cardiovascular anomaly, pure venous blood or mixed venous arterial blood mixed with venous and arterial blood can flow throughout the body in the left ventricle of the heart.
• In this case, cyanosis may develop all over the body, resulting in cyanosis of the lips, tongue, under fingernails and other parts of the body. As such, congenital cardiovascular anomalies that may accompany systemic cyanosis are called systemic cyanotic congenital cardiovascular malformations.
• Normal blood circulation is when venous blood in the right atrium passes through the three-thousand plate, passes through the right ventricle, through the pulmonary artery, and then into the lungs.
• However, when venous blood in the right atrium passes through the right ventricle and does not flow into the lungs through the pulmonary artery, it flows into the left atrium through an atrial septal defect and then circulates throughout the body. ) may occur.
• Congenital cardiovascular anomalies that do not result in central cyanosis are called non-cyanotic congenital cardiovascular malformations.
• In other words, a congenital cardiovascular anomaly in which the heart can pump arterial blood throughout the body and central cyanosis does not occur in the skin or mucous membrane is called a cyanotic congenital cardiovascular anomaly.
Signs, symptoms of congenital cardiovascular malformations
• Symptoms and signs differ depending on the degree and type of congenital cardiovascular anomaly, the presence or absence of complications due to a congenital cardiovascular anomaly, and age.
• These days, most of the congenital cardiovascular anomalies are due to the fact that, after being born in a hospital delivery room, most newborns are given care in the neonatal room and receive at least one or two detailed newborn health check-ups from a pediatrician before being discharged home. It is common to receive a diagnosis and receive appropriate treatment at the time of a newborn health checkup in the neonatal room.
• Even if you were not diagnosed with a congenital cardiovascular anomaly during the newborn health checkup in the neonatal unit, the first regular health checkup 3 to 14 days after being discharged from the neonatal unit at the pediatric department or from birth to puberty It is normal for children and adolescents (0-18 years old) to receive regular health check-ups until they become It is common to be able to diagnose congenital heart anomalies in newborns or infants who have had them since birth and to receive appropriate treatment at an early stage.
• Certain types of congenital cardiovascular anomalies are congenital but may not cause any symptoms.
• Parents are unaware that their child has any congenital cardiovascular anomalies, and that they have congenital cardiovascular disease when they first hear an abnormal heart murmur during a health check-up at the pediatric department or during regular school health check-ups due to some other disease. In some cases, the facts are diagnosed for the first time.
• In most cases of severe congenital cardiovascular anomalies, symptoms resulting from the congenital cardiovascular anomaly appear soon after birth.
• For this reason, it is common to be diagnosed early after birth to have a congenital cardiovascular anomaly.
• Occasionally, a neonatal congenital cardiovascular malformation may not be diagnosed. However, when there is a severe congenital cardiovascular anomaly, in most cases, various symptom signs appear from the time of newborn, so it is usually first diagnosed with severe congenital cardiovascular anomaly before 1 to 2 months of age.
• Severe congenital cardiovascular anomalies may present symptomatic signs of rapid pulse, frequent breathing, and a pale face in newborns and infants.
• It takes a long time to suck and eat because it is difficult to suck on milk or artificial nutrition.
• You may not gain weight well, may be stunted, and look lifeless. Diagnosis of congenital cardiovascular malformations
• If the congenital cardiovascular disease is suspected based on medical history, symptom signs, and examination findings, chest X-ray, electrocardiogram, cardiovascular ultrasound, nuclear cardiology examination, cardiovascular MRI, cardiac catheter examination, and other various It can be diagnosed by any type of test.
• Diagnosis methods differ depending on the type, severity, presence of complications, and age of congenital cardiovascular anomalies.
• Some children with mild congenital cardiovascular malformations may live a lifetime of health without even knowing they have congenital cardiovascular malformations.
• Among children with severe congenital cardiovascular anomalies, some children suffer from congenital cardiovascular anomalies, which prevent them from performing their normal daily activities and suffer from complications caused by congenital cardiovascular disease.
• In some cases, severe congenital cardiovascular anomalies in newborns survived after receiving emergency diagnosis and treatment in the neonatal unit and follow-up emergency surgery in the neonatal intensive care unit of a general hospital.
• chest x-ray, electrocardiography, echocardiogram (echocardiogram), cardiac catheterization (cardiac catheterization), echocardiography (phonocardiogram), and, or It can be confirmed by several other tests.
• It is basic to examine the heart by examination, palpation, percussion, and auscultation before making a diagnosis with these tests.
• These days, the medical technology for diagnosing congenital cardiovascular disease has been remarkably developed, so it is common to easily diagnose severe congenital heart anomalies on the very day of birth.
• Congenital vascular malformations can also occur in the aorta or pulmonary artery attached to the heart.
• What kind of malformation occurs in the heart valve, etc., where the origin of the aorta or pulmonary artery is attached. If any part of the aorta or pulmonary artery is malformed, what is the size of the malformation, what is the anatomy of the malformation, You can accurately diagnose whether the function is normal, etc.
• Depending on the detailed diagnosis results, congenital cardiovascular malformations or aortic or pulmonary arterial malformations can be effectively treated.
• Most congenital cardiovascular anomalies can be cured with relatively safe and easy surgery.
• However, some congenital cardiovascular malformations cannot be cured.
• For congenital cardiovascular anomalies that cannot be cured, palliative surgery treatment is used to restore normal cardiovascular function. Congenital cardiovascular anomalies must be diagnosed early and appropriately treated at an early stage.
• Pulse oximetry detects heart defects in newborns. Source: : Contemporary Pediatrics eConsult, May 17, 2012.
Picture 16. Congenital heart anomaly can be diagnosed by medical history, symptom signs, and examination Copyright ⓒ 2011 John Sangwon Lee, MD, FAAP
Picture 17. Chest X-rays are very helpful in diagnosing congenital heart anomalies. The white area in the red circle is the heart Copyright ⓒ 2011 John Sangwon Lee, MD, FAAP
Figure 20. Cardiac catheterization through the inferior vena cava (cardiac catheterization, cardiac catheterization) Copyright ⓒ 2011 John Sangwon Lee, MD, FAAP
Figure 21. Cardiac catheterization through the superior vena cava (cardiac catheterization, cardiac catheterization) a-left atrium, b-his ventricle, c-left ventricle, d-right ventricle, e-3 top plate, f-right atrium, g-sinus node Copyright ⓒ 2011 John Sangwon Lee, MD, FAAP
Treatment of congenital cardiovascular malformations
• Treatment is different depending on the size, symptom signs, types, complications, and age of the congenital heart anomaly.
• A very small ventricular septal defect, a very small ductus duct in a premature infant, and any other congenital cardiovascular anomaly may resolve spontaneously without cardiac surgery.
• Sometimes you can live a normal life with the congenital cardiovascular anomaly without any symptoms and no treatment required.
• If the Department of Pediatrics is diagnosed with any type of congenital cardiovascular anomaly, you should receive a more definitive diagnosis and treatment from a pediatric cardiologist soon.
• There may be congenital anomalies of the cardiovascular system, or there may be congenital anomalies such as the origin of the aorta of the left ventricle or the origin of the pulmonary artery of the right ventricle. At this time, the abnormality should be diagnosed in more detail in which part of the origin of the heart.
• whether the congenital cardiovascular anomaly should be treated with heart surgery;
• Whether you need treatment for heart surgery;
• whether it can be cured with heart surgery;
• It is necessary to quickly learn more about the treatment of congenital cardiovascular malformations, such as whether it can be cured by receiving primary heart surgery treatment, whether it can be cured by receiving secondary heart surgery treatment, and whether there is no possibility of being cured even with cardiac surgery treatment.
• When, where, and from which pediatric cardiologist you will receive surgery for heart surgery;
• What medications to take prophylactic treatment prior to surgery;
• What is the success rate of cardiac surgery treatment;
• How much does it cost to treat heart surgery;
• The prognosis after surgery is:
• Parents and children with congenital cardiovascular malformations should know as soon as possible about precautions, etc.
• Whether you can get medical bills from the national social welfare insurance. • Parents should at least have more medical knowledge than would have to be a psychiatrist on pediatric congenital cardiovascular anomalies.
• When congenital cardiovascular anomalies are treated with surgery, pediatric cardiologists, pediatric cardiologists, pediatricians and other specialists, nurses specializing in pediatric cardiovascular anomalies, clinical pathologists, etc. It is common to become a member of a malformation treatment team and participate in a successful operation.
• For this reason, surgery for congenital cardiovascular anomalies cannot be performed in any hospital and is usually only performed in a few general hospitals nationwide.
• For more information on congenital cardiovascular disease, refer to each of the following sections.
• Ivabradine (Corlanor), which is used to treat heart failure in adults, is sometimes used to treat heart failure in children. Source: AAP News 6/2019 Sources and References
• Ventricular septal defect
• Atrial septal defect
• Patent ductus arteriosus
• Coarctation of aorta
• Aortic stenosis
• Pulmonary stenosis
• Tetralogy of Fallot
• Tricuspid atresia • Aortic transposition (Transposition of the great arteries)
The following is an example of Internet pediatric health consultation Q&A regarding “atrial septal defect, ventricular atrial septal defect, congenital heart anomaly, left hydronephrosis”.
Q&A.Atrial septal defect, ventricular atrial septal defect, congenital heart anomaly, left hydronephrosis
Q. Hello? I am a 29-year-old male living in Japan. No other than that, my wife Ora (Japanese) gave birth to a baby boy on August 12th, and she was diagnosed with ventricular/atrial septal defect and hydronephrosis at the hospital. A ventricular septal defect is located just below the pulmonary artery, and an atrial septal defect has located some distance from the aorta. The size of the perforation of the atrial septal defect has not yet been clearly diagnosed, but the ventricular septal defect was measured to be 6 mm in width and 3 mm in length.
Hydronephrosis was diagnosed as having an abnormal size on one side of the left kidney, and it is said to be 1.5 to 1.8 times that of the right kidney. The hydronephrosis was checked by ultrasound before childbirth, so I decided to make a treatment plan while watching the progress.
Cardiac anomalies were checked during a work-up for a kidney test after childbirth etc – I found out I was pregnant in the 5th month of pregnancy and went to the hospital (there was no morning sickness at all). – The mother did not think that amenorrhea was pregnancy and did not go to the hospital for treatment. – No basic fetal examination was performed in the 1st or 2nd month of pregnancy (check for various abnormalities, etc.). – There were two episodes of reverse childbirth at 24 and 30 weeks. – I was hospitalized 3 weeks before the expected date of delivery and was preparing for a cesarean section while checking the heart rate of the fetus.
After the 3rd sudden cardiac increase, a cesarean section was performed under the doctor’s diagnosis. Baby’s current state (day 8) – No abnormal urination – No abnormalities in vital signs such as blood pressure and heart rate (diagnosed by the hospital) – There is a phenomenon that the heart rate falls below 100 for 1 to 2 minutes once a day – I can’t get enough breast milk on my own. You can only suck up to 5cc of breast milk at a time. –
Artificial oil is fed 40-50cc at a time 4-5 times a day – There were cases in which I slept without eating even during the feeding time (no matter how much the nurse woke me up, I did not wake up) It’s been a while, but I’m really worried that abnormalities not only in the kidneys but also in the heart are found. We are fortunate to have found it early, but it is truly heartbreaking that it is not painful for a newborn.
The medical staff in this department set the surgery as the worst case and informed me of the treatment plan to conduct a detailed examination while monitoring the progress in the next two to three weeks. I was told to be safe while listening to a lot of things, and personally browsing the website, I tried to find out in a floating way, but again, considering that there are two septal defects in the ventricle and atrium, the possibility of surgery is increasing. Although it may be good to have a newborn baby undergo surgery in the end, it is very insecure and pitiful for the new mom and dad. Would it be okay? What should I prepare for in the future?
A. to Daddy Hello. Thank you very much for your good questions and detailed medical history. Thank you once again for giving your family medical history, past medical history, pregnancy history, childbirth process, diagnosis, etc. Congratulations on the birth of your baby girl. A baby with such wonderful parents will soon receive the glory and blessings of her God and will soon recover.
I can’t tell you how happy and contented it was to see the children who had very severe congenital cardiovascular malformations grow up healthy and normal after undergoing cardiovascular anomaly treatment surgery. These are my experiences at Yale University School of Medicine Pediatrics Hospital, Uconn School of Medicine, Department of Pediatrics, and Hartford Hospital.
Nowadays, most congenital cardiovascular anomalies can be accurately diagnosed at an early stage and can be cured relatively easily with surgery and medical treatment to treat congenital cardiovascular anomalies, and follow-up treatment can be done well after surgery. Seriously ill children or parents themselves can develop FAGS syndrome, but don’t worry too much and follow your doctor’s instructions to continue caring for and treating you and pray.
I believe that Mr. Daddy, whether a non-medical parent or a physician, is well versed in medicine, especially pediatrics. I would like to say a few things. I will also do more research and organize after receiving questions. atrial septal defect significantly Nanwongong opening, secondary hole defect, It is classified as an endocardial ridge defect. (see Atrial Septal Defect) The foramen is not a congenital heart anomaly. It is normal for the foramen ovale to block spontaneously unless there is pulmonary artery occlusion or tricuspid valve occlusion, and there is no congenital cardiovascular malformation in the right ventricle.
Occasionally, the patency of the foramen fora can remain for a lifetime and is not a health problem. Depending on the size and symptom signs of secondary foramen or supramial defects, you should seek immediate treatment from a pediatrician, pediatric cardiologist, pediatric cardiologist, and other specialists.
We need to know what causes left hydrocephalus. If there is a congenital anomaly in one system of the body, it is possible that another type of birth defect is present in another system of the body. For example, a child with Down syndrome may have a congenital cardiovascular malformation and may have bladder urethral reflux, which may result in hydronephrosis.
Please receive an appropriate diagnosis and treatment for him. How would you like to try this treatment? Nutrients must be properly ingested to avoid any abnormalities in nutrients, water, and electrolytes. It would be nice to have the help of a pediatric nurse and nutritionist. Find out if you have anemia.
As you know, if you have congenital cardiovascular anomalies, especially systemic cyanosis, it is normal for the hemoglobin concentration to be higher than that of newborns or infants who do not have cardiovascular anomalies. For that reason, even if your hemoglobin level is normal, you may still have anemia. Congenital cardiovascular anomalies may result in systemic cyanosis. If you have systemic cyanosis, you may need oxygen-breathing therapy.
If you have systemic cyanosis, your red blood cell count may be higher than normal. You may develop heart congestion and may be more susceptible to infectious diseases such as pneumonia. You are more likely to get endocarditis when you have surgery on parts of the body that are in the digestive or other systems, such as the mouth. Therefore, antibiotic prophylaxis should be taken.
You should also consider consulting a geneticist and chromosomal testing to determine the cause of congenital cardiovascular anomalies and hydronephrosis. With the help of a pediatric specialist, a pediatric nephrologist, and a pediatric nephrologist, you need to find out the cause of hydronephrosis, perform the necessary tests to diagnose various urinary system diseases, and receive appropriate treatment accordingly. Preventive treatment should be taken to avoid getting a urinary tract infection.
Various basic immunizations should be received according to age and timing. If possible, we recommend that you purchase various types of health insurance. We recommend that you discuss any health issues with your baby in consultation with your pediatrician. In addition to the above, there are many more special things to do for your little one. If you need more, please consult with your regular pediatrician.
As you may know, I am a general pediatrician. In the Department of Pediatrics, there is a general Department of Pediatrics, and a Pediatric Specialist is divided into a Pediatric Specialist of each branch who has studied and studied pediatrics more specifically according to each system in the body. A general pediatrician specializes in general pediatrics related to pediatrics. A pediatric cardiologist who specializes in general pediatrics and pediatrics related to the pediatric heart is called a pediatric cardiologist. In general, if a pediatric cardiologist has any further questions about pediatric cardiovascular disease, they can consult a pediatric cardiologist who specializes in pediatric cardiology and see the child. It is a medical practice these days for surgeons to consult a pediatric cardiac surgeon who specializes in pediatric cardiac surgery and receive counseling and treatment for pediatric cardiovascular disease surgery. In addition to the above, there are many more special tasks to be done for your child, so please consult with your pediatrician. In addition, there are pediatric anesthesiologists who mainly specialize in pediatric anesthesia when children undergo surgery, and there are pediatric nurses who specialize in treating children’s diseases.
In addition, there are pediatric hospitals where only children and adolescents are hospitalized and treated, and there are pediatric hospitals and pediatric hospitals with staff that can handle all issues related to the well-being of children and adolescents more effectively.
The reason I say this is to help you select the right medical staff and hospital. I would appreciate it if you could let me know the results of your treatment to help me learn. If you have any further questions, please feel free to contact us again. thank you. Lee Sang-won.
출처 및 참조 문헌 Sources and references
- NelsonTextbook of Pediatrics 22ND Ed
- The Harriet Lane Handbook 22ND Ed
- Growth and development of the children
- Red Book 32nd Ed 2021-2024
- Neonatal Resuscitation, American Academy Pediatrics
- www.drleepediatrics.com 제1권 소아청소년 응급 의료
- www.drleepediatrics.com 제2권 소아청소년 예방
- www.drleepediatrics.com 제3권 소아청소년 성장 발육 육아
- www.drleepediatrics.com 제4권 모유,모유수유, 이유
- www.drleepediatrics.com 제5권 인공영양, 우유, 이유식, 비타민, 미네랄, 단백질, 탄수화물, 지방
- www.drleepediatrics.com 제6권 신생아 성장 발육 육아 질병
- www.drleepediatrics.com제7권 소아청소년 감염병
- www.drleepediatrics.com제8권 소아청소년 호흡기 질환
- www.drleepediatrics.com제9권 소아청소년 소화기 질환
- www.drleepediatrics.com제10권. 소아청소년 신장 비뇨 생식기 질환
- www.drleepediatrics.com제11권. 소아청소년 심장 혈관계 질환
- www.drleepediatrics.com제12권. 소아청소년 신경 정신 질환, 행동 수면 문제
- www.drleepediatrics.com제13권. 소아청소년 혈액, 림프, 종양 질환
- www.drleepediatrics.com제14권. 소아청소년 내분비, 유전, 염색체, 대사, 희귀병
- www.drleepediatrics.com제15권. 소아청소년 알레르기, 자가 면역질환
- www.drleepediatrics.com제16권. 소아청소년 정형외과 질환
- www.drleepediatrics.com제17권. 소아청소년 피부 질환
- www.drleepediatrics.com제18권. 소아청소년 이비인후(귀 코 인두 후두) 질환
- www.drleepediatrics.com제19권. 소아청소년 안과 (눈)질환
- www.drleepediatrics.com 제20권 소아청소년 이 (치아)질환
- www.drleepediatrics.com 제21권 소아청소년 가정 학교 간호
- www.drleepediatrics.com 제22권 아들 딸 이렇게 사랑해 키우세요
- www.drleepediatrics.com 제23권 사춘기 아이들의 성장 발육 질병
- www.drleepediatrics.com 제24권 소아청소년 성교육
- www.drleepediatrics.com 제25권 임신, 분만, 출산, 신생아 돌보기
- Red book 29th-31st edition 2021
- Nelson Text Book of Pediatrics 19th- 21st Edition
- The Johns Hopkins Hospital, The Harriet Lane Handbook, 22nd edition
- 응급환자관리 정담미디어
- Pediatric Nutritional Handbook American Academy of Pediatrics
- 소아가정간호백과–부모도 반의사가 되어야 한다, 이상원 저
- The pregnancy Bible. By Joan stone, MD. Keith Eddleman, MD
- Neonatology Jeffrey J. Pomerance, C. Joan Richardson
- Preparation for Birth. Beverly Savage and Dianna Smith
- 임신에서 신생아 돌보기까지. 이상원
- Breastfeeding. by Ruth Lawrence and Robert Lawrence
- Sources and references on Growth, Development, Cares, and Diseases of Newborn Infants
- Emergency Medical Service for Children, By Ross Lab. May 1989. p.10
- Emergency care, Harvey Grant and Robert Murray
- Emergency Care Transportation of Sick and Injured American Academy of Orthopaedic Surgeons
- Emergency Pediatrics A Guide to Ambulatory Care, Roger M. Barkin, Peter Rosen
- Quick Reference To Pediatric Emergencies, Delmer J. Pascoe, M.D., Moses Grossman, M.D. with 26 contributors
- Neonatal resuscitation Ameican academy of pediatrics
- Pediatric Nutritional Handbook American Academy of Pediatrics
- Pediatric Resuscitation Pediatric Clinics of North America, Stephen M. Schexnayder, M.D.
-
Pediatric Critical Care, Pediatric Clinics of North America, James P. Orlowski, M.D.
-
Preparation for Birth. Beverly Savage and Dianna Smith
-
Infectious disease of children, Saul Krugman, Samuel L Katz, Ann A.
- 제4권 모유, 모유수유, 이유 참조문헌 및 출처
- 제5권 인공영양, 우유, 이유, 비타민, 단백질, 지방 탄수 화물 참조문헌 및 출처
- 제6권 신생아 성장발육 양호 질병 참조문헌 및 출처
- 소아과학 대한교과서
Copyright ⓒ 2020 John Sangwon Lee, MD., FAAP
“부모도 반의사가 되어야 한다”-내용은 여러분들의 의사로부터 얻은 정보와 진료를 대신할 수 없습니다.
“The information contained in this publication should not be used as a substitute for the medical care and advice of your doctor. There may be variations in treatment that your doctor may recommend based on individual facts and circumstances.
“Parental education is the best medicine.